There are two things in Emergeceny Medicine that scare me: 1) babies and 2) airway obstruction. So I thought I’d write a short post on what happens when you combine the two! Today its about Stridor in children under 6 months. Its something that uncommonly presents to the ED, but when it does you need to be confident in how to manage and diagnose the cause. Remember stridor is a symptom NOT a diagnosis.
Imagine you are the ED doc working in a rural ED. The parents of 4month baby Stanley rush him into the department, “Doc he’s making a really funny noise, help!”. What are you going to do next? Whats the diagnosis? Oh and as there is no ENT surgeon in the hospital, how are you going to transfer him if he needs to see one?
Stridor: A high pitched sound produced by turbulent airflow through a narrow, partially obstructed airway. As air is pushed through a narrow tube there is decreased lateral pressure. This causes the airway walls to collapse and vibrate, otherwise known as stridor.
Remember this from physics?
So if you reduce the radius by 1/2, the resistance is increased 16 fold! In Kids, 1mm of oedema can reduce the cross-sectional area of their airway by 50%. A small amount of reduction can cause significant problems for them and you!.
It can be difficult to hear the stridor, especially in babies, and parents may describe it as a “wheeze”. Clarify what they mean by a “wheeze’ and whether its inspiratory, expiratory or both.
-
Inspiratory stridor suggests a laryngeal obstruction
-
Expiratory stridor implies tracheobronchial obstruction
-
Biphasic stridor suggests a subglottic or glottic anomaly
In children under 6 months, the commonest cause of stridor is congenital. They usually need direct visualisation via an endoscope.
Laryngomalacia:
The commonest cause of congenital stridor in neonates. It’s caused by a delay in the maturation of the structures that support the larynx. This gives rise to an “omega” shaped larynx. The epiglottic and aryepiglottic folds collapse during inspiration causing obstruction. This usually resolves by 18 months. It can be exacerbated by a respiratory tract infection or increased work of breathing. It can lead to failure to thrive, apnoea and pulmonary hypertension which will need surgical intervention. 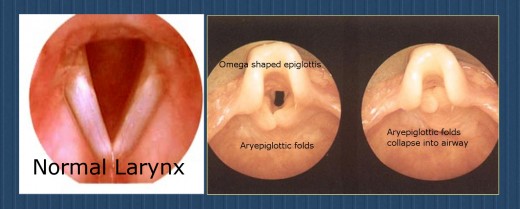 Vocal Cord Paralysis:
Vocal Cord Paralysis:
Unilateral cord paralysis is more common and presents with stridor, hoarse voice and cry changes. Bilateral cord paralysis children have a normal voice with stridor. They are at risk of cyanosis and apnoea. A flexible nasoendoscopy is the diagnostic method of choice. Endotracheal intubation can be difficult and you need to be ready to do a needle cricothyroidotomy if needed, after which a tracheotomy is then required.
Subglottic Stenosis (SGS): The subglottic airway is narrowest part of the airway. This is because it is a complete, nonexpandable, and nonpliable ring, unlike the trachea, which has a posterior membranous section, and the larynx, which has a posterior muscular section. Congential SGS is diagnosed in the first few months of life after a persistent inspiratory stridor is heard. Acquired SGS is usually due to prolonged endotracheal intubation in premature babies. In most cases the symptoms usually resolve in the first few years of life.

4month old with SGS born at 26/40 and had 3months of ETT intubation. (Courtesy of emedicine.medscape.com)
Haemangiomas:
Now we are getting into the rare stuff…. However I’m all about “Sweating the small stuff”. Knowledge is power and if you don’t think of it, you won’t know to look for it! Haemangiomas a benign congenital tumours of endothelial cells of vascular malformations. They usually appear and enlarge in the first year of life. Most (80%) are located above the clavicle, including the airway causing stridor. Uncover the child fully and look for them! It may give you a clue as to the cause of the stridor. They can be reduced in size with steroids, laser or surgery. They will bleed….. A LOT if you are not careful when intubating with the ETT.

Vascular Slings and Rings:
Now these are rare! Congenital anomalies of the aortic arch and pulmonary artery can cause anomalous vessels to constrict the trachea or oesophagus. These manifest in a stridor from birth which becomes exaggerated during a respiratory tract infection. CT angiography and bronchoscopy are used to evaluate them. These kids need surgery as their definitive treatment.
Eg of a Double Aortic Arch causing tracheal compression:


So lets get back to baby Stanley:
As you get mum to sit on the trolley bed and hold him, he settles and the stridor becomes less marked. He was a term baby and is otherwise fit and well but has been coryzally recently and had a “funny turn” where he went blue for a minute or so. There are no haemangiomas that you can see. His sats are 93% on room air and he’s tachycardic. The oxygen mask makes him more agitated and so you decide to tell mum just to hold it in front of his face. He needs an urgent ENT review +/- an endoscopy to look for the cause of the stridor. The nearest ENT surgeon is an 1hr away by road and its 2am. Stanley needs to be transferred with an experienced anaesthetist with a Plan A,B,C in place. As you are in a rural ED, there may not be a paediatric anaesthetist available, get the anaesthetic SpR to call their consultant in and you call the ED consultant and the paediatricians call theirs. You need to call for help early! Think about a retrieval service if there is one. Does he need to be intubated prior to transfer or do you hold out until he gets to the urban ED? If you choose to intubate, how would you do it?…..Inhalational induction? There is a great post on how to manage the airway in these patients and the South Thames Retrieval Service have some excellent guidelines including on intubation.
Luckily you can call a retrieval service to come and take Stanley to the urban hospital. He had an inhalational induction ETT intubation followed by a a tracheostomy. He was diagnosed with bilateral vocal cord paralysis.
In Summary:
1) Get help early from senior clinicians.
2) Not only keep the baby and parents calm, but keep yourself calm. And as Fred Shreo says: ” You want to be like a duck: calm above the water and paddling like hell underneath!”

3) Use the Power of Negative Thinking. Astronaut Cmdr Chris Hadfield said: “I’m pretty sure that I can deal with what life throws at me because I’ve thought about what to do if things go wrong, as well as right. That’s the power of negative thinking.” This philosophy can help you out everyday at work. It certainly has helped me on numerous occasions!
KR
N
