Hope fully a short blog today! In the spirit that we should “sweat the small stuff”, I thought i’d talk about ECGs. How confident are you of reading them? I agree with Amal Mattu‘s mantra that Emergency Physcians should be as good as or better at reading ECG’s than cardiologists as we probably look at more of them on a daily basis. So you are working in the ED, sitting at a desk and writing your notes. A nurse comes up to you and asks you to look at an ECG of 70yrold male with chest pain. “He’s a bit sweaty….”
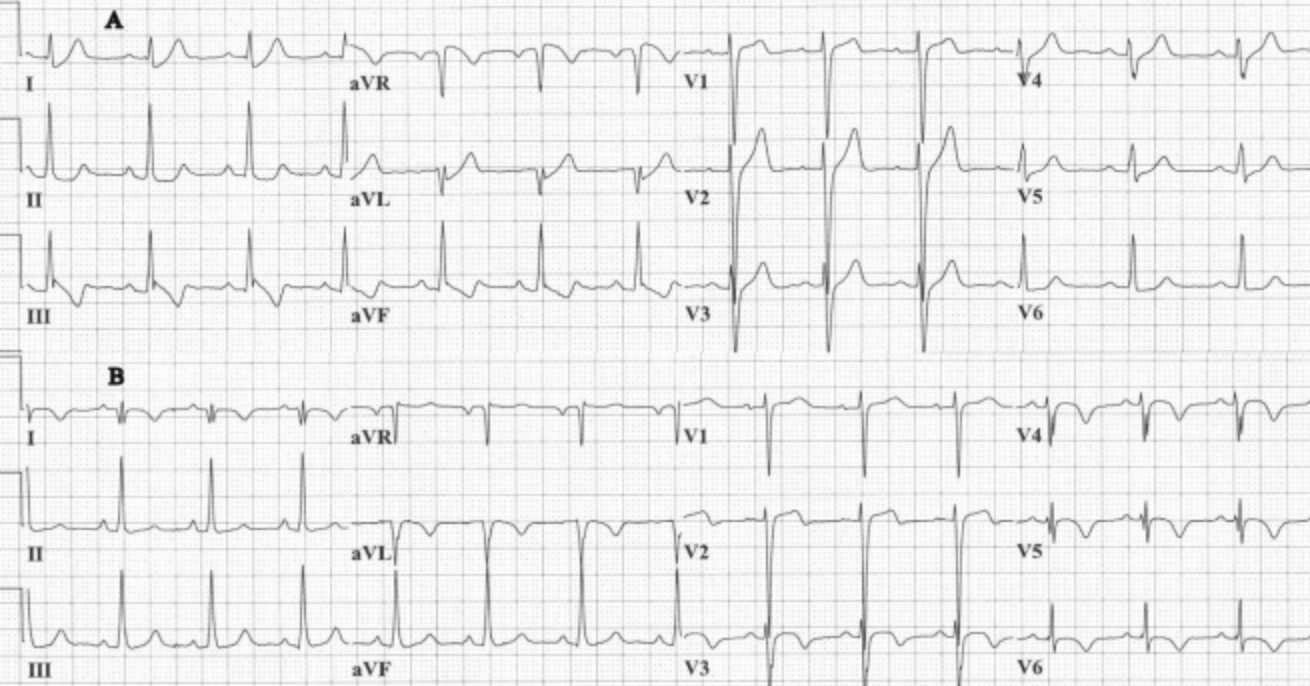
Now there is T wave inversion in III and AVF and after looking at the patient you send him to resus and treat him for ACS. He starts to feel better. His troponin is raised and he is moved to the wardto await a cardiology review several hours later. Feeling pretty chuffed with yourself, you high five the resus nurse. Just as the “high five” ends another patient is wheeled into resus with chest pain. Its a 40 yrold lady with SOB and chest pain. The paramedic says ” sorry doc, can you look at this ECG?”.
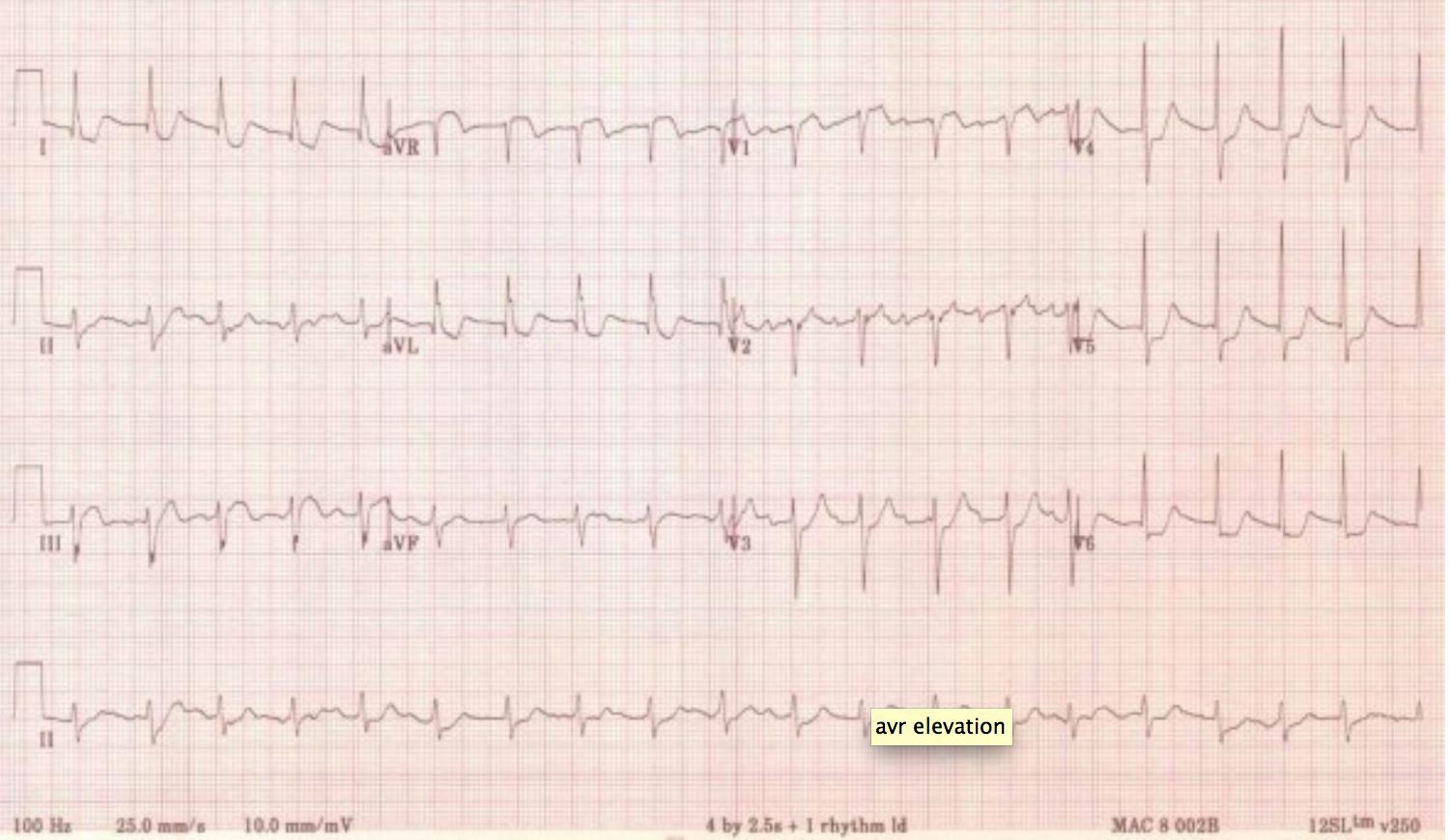
 You’re feeling awesome and confident, a cursory look at the ECGshows ischaemic changes in the lateral leads with some biphasic T waves. You look at the patient who appears in some discomfort. She settles with some morphine and you start on the ACS protocol. “Chest pains are a doddle…..” you think to yourself. A day later the medical registrar says to you ” do you remember that patient from yesterday?….” (one of the worst words to hear in medicine…listen to Brian Goldman’s TED talk “Doctors make mistakes..”) Both patients were able to have an angiogram on the same day which showed extensive LAD/ LMCA disease, unfortunately the 70 yrold male patient died overnight. You wonder if there was anything different you could have done to change his outcome? Have a look at the ECG’s again, paying closer attention to AVR. Both show ST elevation. In the context of patients with chest pain, ST elevation in AVR is indicative of proximal LAD/ LMCA disease. If there is ST elevation in AVR and
You’re feeling awesome and confident, a cursory look at the ECGshows ischaemic changes in the lateral leads with some biphasic T waves. You look at the patient who appears in some discomfort. She settles with some morphine and you start on the ACS protocol. “Chest pains are a doddle…..” you think to yourself. A day later the medical registrar says to you ” do you remember that patient from yesterday?….” (one of the worst words to hear in medicine…listen to Brian Goldman’s TED talk “Doctors make mistakes..”) Both patients were able to have an angiogram on the same day which showed extensive LAD/ LMCA disease, unfortunately the 70 yrold male patient died overnight. You wonder if there was anything different you could have done to change his outcome? Have a look at the ECG’s again, paying closer attention to AVR. Both show ST elevation. In the context of patients with chest pain, ST elevation in AVR is indicative of proximal LAD/ LMCA disease. If there is ST elevation in AVR and
- ST elevation in AVL: LMCA occlusion
- ST elevation in V1: LMCA/proximal LAD occlusion
- ST Elevation in AVR > STE in V1: LMCA occlusion
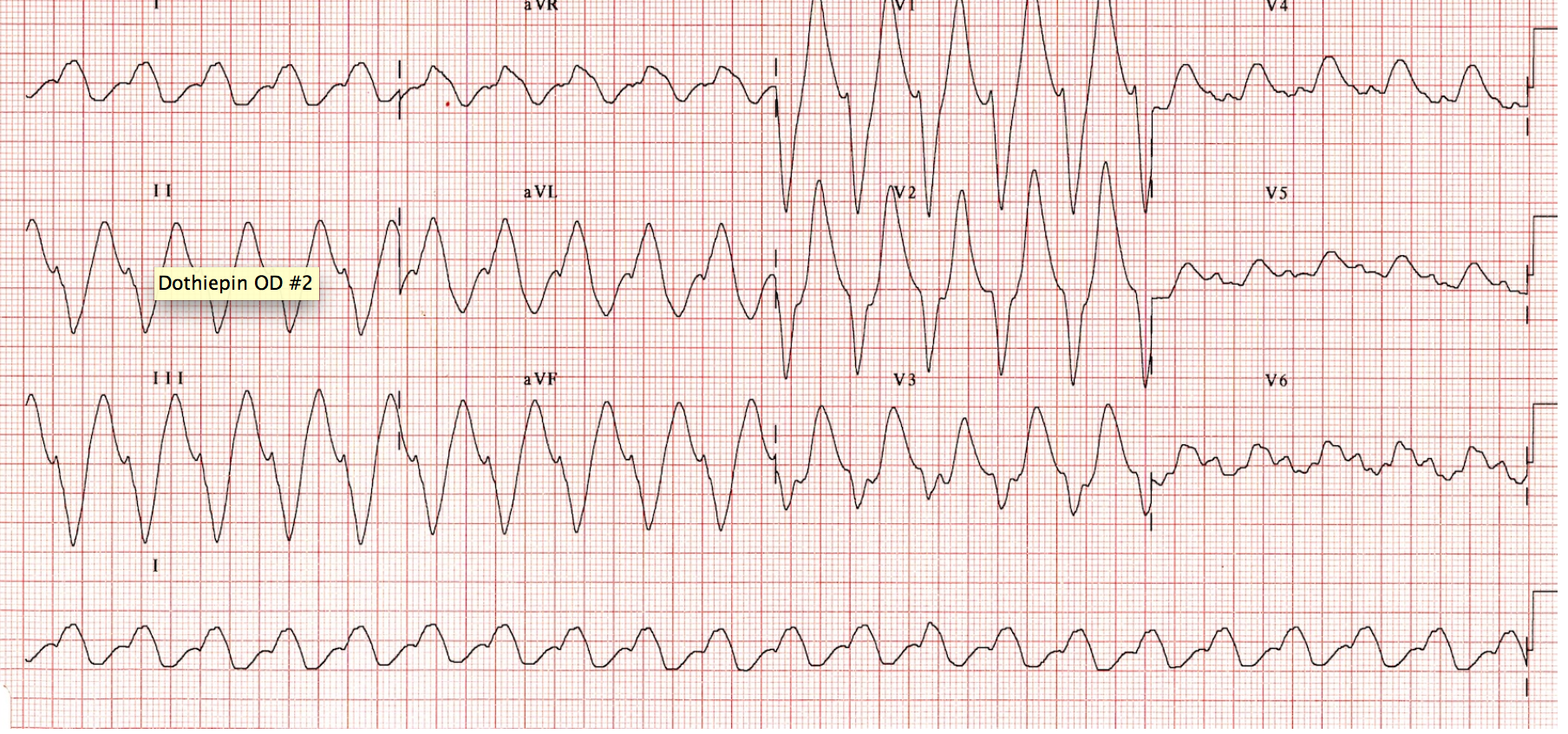
LMCA occlusion has a high mortality rate and patients often require a CABG. Time to PCI is the only predictor of survival. 70% mortality without immediate PCI. (Courtesy of Amal Mattu). Bottom line is ST Elevation in AVR with ACS patients have a high mortality rate. The “red phone” rings…..” 20yrol male, reduced GCS ETA 10mins”….. He comes in being ventilated with an IGEL. He is intubated and an ABG shows a pH: 7.14 HCO3-: 12. This is his ECG:
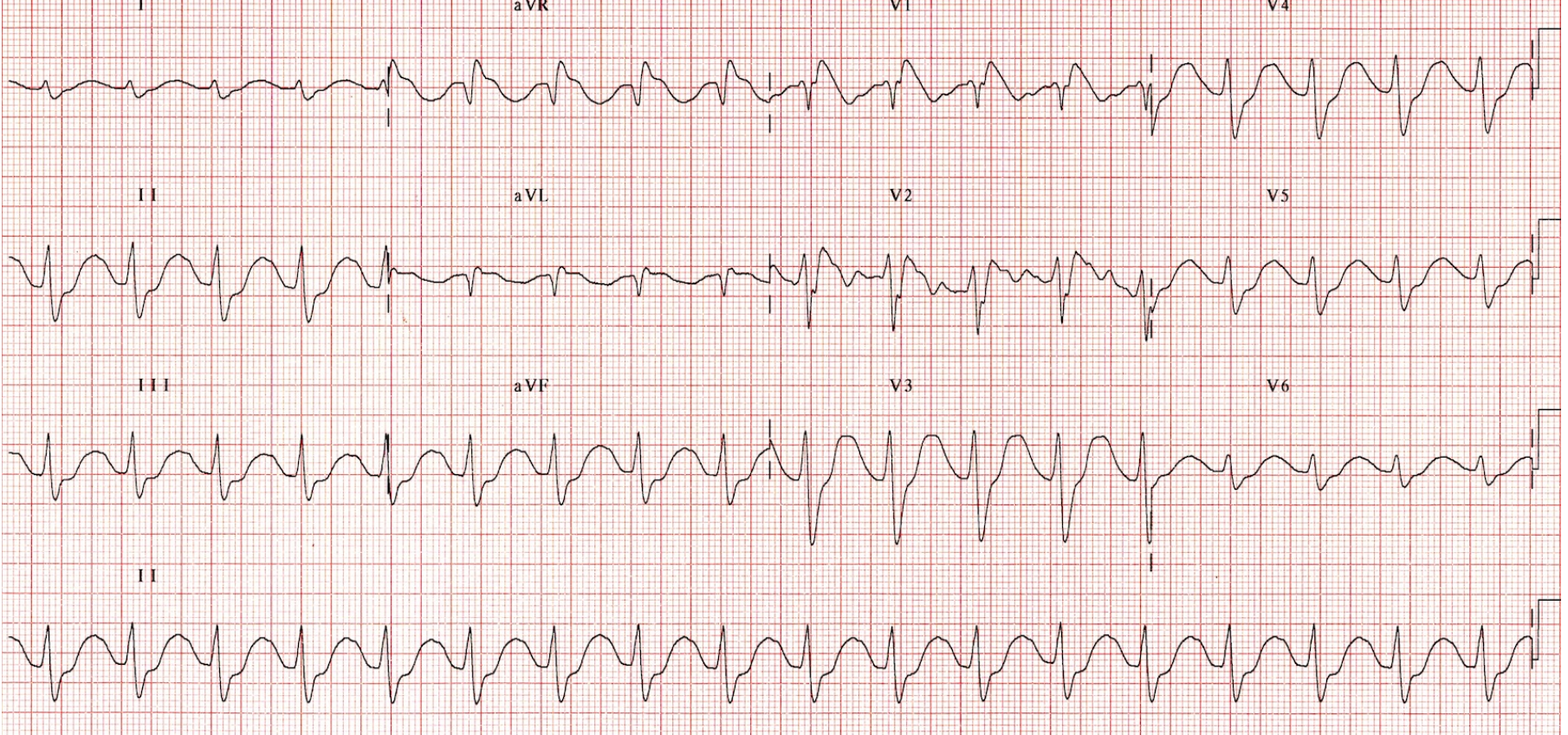
His ECG monitor then changes and a repeat ECG shows this:
You diagnose the patient and treat him. His ECG is now:
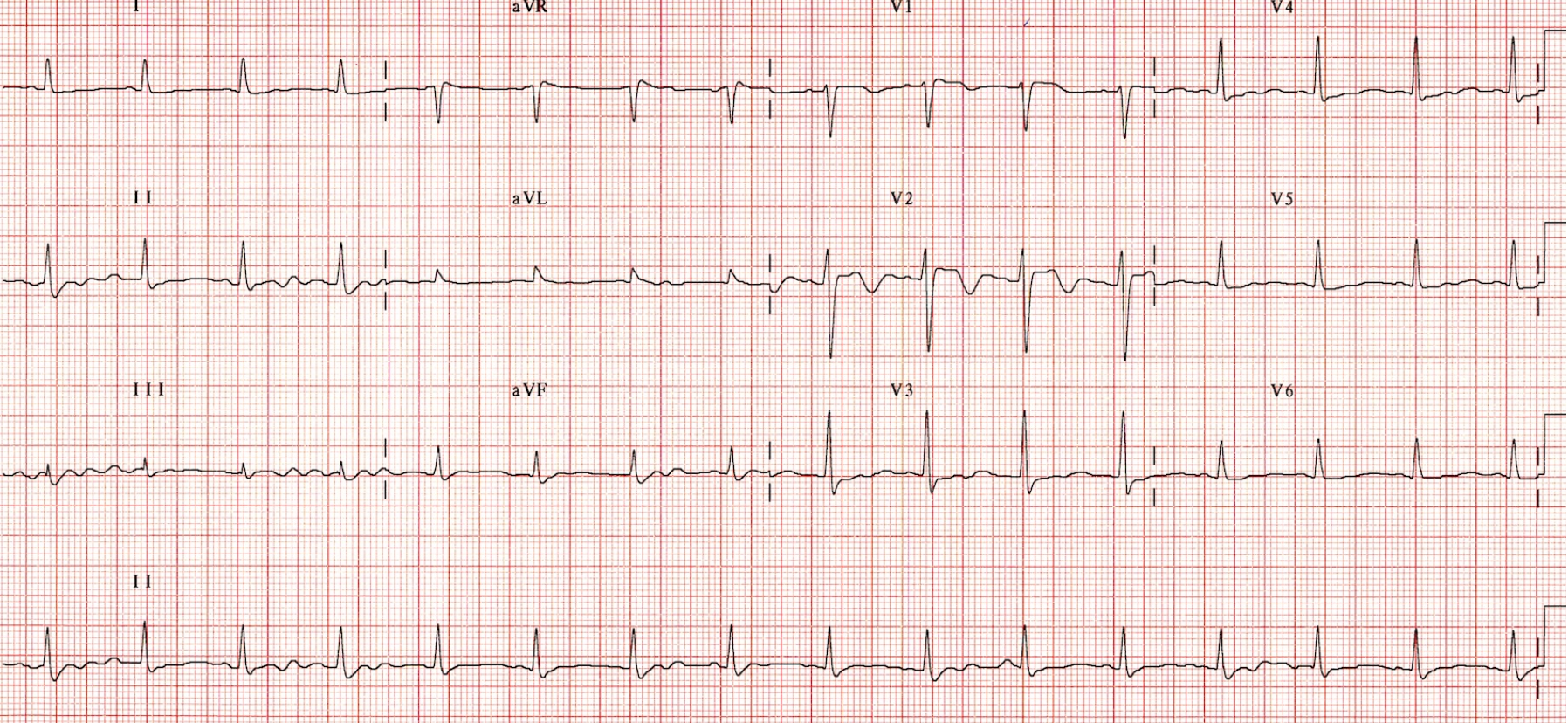
The patient is moved to the ICU and is discharged from hospital a week later. Now for those of you reading this blog that are unsure of the diagnosis, you are probably in the majority. However , the light at the end of the tunnel is that after reading this you will NEVER MISS the diagnosis….. TCA Overdose Again AVR is so important look at. TCA’s are sodium channel blockers and the ECG findings relate to that. In Lead AVR:
- Prolonged QRS: >100ms is predictor of seizures. >160ms is a predictor of VT/VF
- Prolonged QTc (inhibition of K channels)
- Tall R wave (R1) >3mm
- R/S ratio > 0.7mm

A lovely summary is on Life in the Fast Lane. Remember that Hyperventilation and boluses of sodium bicarbonate need to be started until you see narrowing of the QRS complexes and improvement of BP. In summary:
- AVR: ST elevation is indicative of LMCA/LAD disease in ACS patients, who will have a high mortality rate
- AVR: Prolonged QRS is a predictor of seizures and VT in TCA overdoses. There is also a dominant R wave (>3mm) and R/S rail >0.7mm.
- Personally I need to be better at reading ECG’s. (I suspect I’m not the only one who thinks this….)
Hope this has helped!
KR
N

{kind=link}
{kind=link}
{kind=link}